The saddest aspect of life right now is that science gathers knowledge faster than society gathers wisdom – Isaac Asimov
In February 2020, when I originally wrote this post, I stated that:
“there’s a bit of a health panic going on (understatement!). Masks are selling out, and I’ve just seen a post on social media from someone who had to visit five different stores in order to find hand-gel. But how scared should we really be of coronavirus COVID-19? As far as I’m concerned, there are plenty of candidates more deserving of our fear and respect. Here, in no particular order, are nine of the worst.”
It’s now nearly 2 years since I originally wrote this blog post, and a year since I last revisited it. a lot has happened in that time. When I initially wrote this post, COVID didn’t come close to making the list, because at the time, we still thought that quarantine and contact tracing would contain it. The SARS outbreak of 2002, and the 2009 H1N1 swine flu pandemic had lulled us into a false sense of security. Now it’s February 2022 and there are encouraging signs that we are finally coming out of the pandemic. I’ll post on that later. Meanwhile, in no particular order, here are my scariest pathogens.
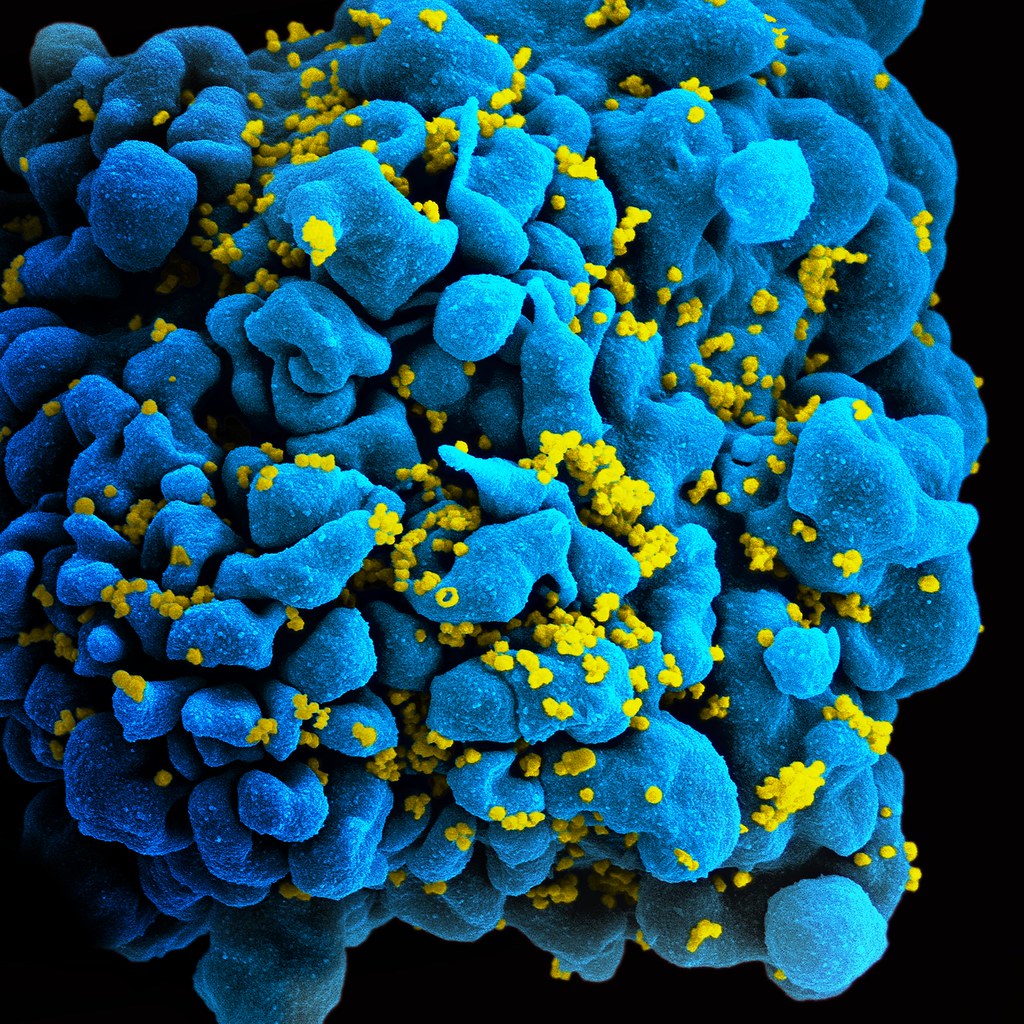
HIV
The human immunodeficiency virus (HIV) attacks the very cells that are meant to defend the body against it. It attacks cells which have the CD4 protein on their surface; these include helper T-cells which play a vital role in the immune system. Over time, the number of circulating helper T-cells decreases; when it drops below a certain level, the immune system effectively fails to function and the patient develops Acquired Immune Deficiency System (AIDS). AIDS has a high mortality rate since patients are unable to fight off serious infections.
But HIV has been conquered, right? Better awareness of the risks of unprotected sex; availability of condoms; provision of clean needles for IV drug users; all of these have helped to slow the spread of the infection. Effective anti-retroviral drugs (ARVs) mean that the disease can now be regarded as chronic; it rarely, if ever, progresses to AIDS.
Well, all of the above apply in developed, Western countries. In the developing world it’s a different story. Condoms are not always widely available, and in certain cultures or religions, their use is forbidden. ARVs are also not necessarily available. In some countries there is denial that HIV is what causes AIDS, meaning that governments refuse to provide access to treatment – this was the case for many years in South Africa.
But in the West we are OK, right? Wrong. HIV is a retrovirus, which means it writes its own DNA into that of infected cells. This means that it can never actually be eliminated from the body, and those infected must take ARVs throughout their lifetime. HIV also mutates rapidly, meaning that it develops resistance; new ARVs must be constantly developed to keep ahead of it. The fact that HIV continues to spread rapidly and go untreated helps it to keep mutating. How long can the drug developers keep ahead of it?
Malaria

Malaria is caused by a plasmodium, a single-celled parasite spread through mosquito bites. According to the World Health Organisation (WHO), in 2018 there were approximately 228 million cases of malaria, with around 405,000 deaths. Malaria has a significant economic impact on countries where it is prevalent due to the cost of healthcare, loss of working days due to illness, and loss of worker productivity due to long-term effects.
The comparatively low death rate is due to the availability of effective anti-malarial drugs. However, malaria is becoming increasingly resistant to anti-malarial drugs, particularly in south-east Asia (Laos, Cambodia and Vietnam) where strains are emerging that are resistant to all currently available treatments. The development of resistant strains is partly due to the fact that organised criminal gangs in some countries are selling sub-standard or counterfeit drugs; these can only be detected using complex laboratory analysis.
A big problem with malaria is that there is no profit to be made from it. Developing new drugs is expensive, and the countries where malaria is prevalent cannot afford to pay the kind of prices big pharmaceutical companies want to charge in order to make a profit. Big pharma are not going to spend millions on developing a new anti-malarial just to make a loss on it, especially if the development of resistance means that after a few years, the drug will be ineffective. So, most of the research into new malaria treatments relies on subsidies from governments, NGOs and charitable donations. For example, one of the newest and most effective anti-malarials made it into clinical use because a partnership with the WHO meant that the manufacturing company could sell it at an affordable price and still make a profit. Fair play to the company concerned though, they did front up a significant amount of money in developing the drug. For the most part though, big pharma are putting their money into those diseases where there is most money to be made, such as cancer, diabetes and cardiovascular disease.
Lack of investment has also impeded development of an effective vaccine against malaria. A vaccine is currently undergoing pilot trials, but as yet there is no data as to how effective it is. Another problem with malaria is that unlike viral or bacterial infections, a patient who has had the disease and recovered does not develop immunity straight away. In fact, it takes multiple attacks of the disease for immunity to build up.
So, why does malaria worry me? Two words: climate change. The reason we don’t have malaria in the UK is that the conditions here are not suitable for the mosquitos which carry the parasite. Historically, malaria was actually very common in Europe and North America. In ancient Roman times, it was so prevalent in the city of Rome that it was known as ‘Roman Fever’. Climate change means that climates are warming up. Increasing incidents of flooding leave behind pools of standing water which may take a long time to drain away, providing a potential breeding ground for the malaria mosquito. As westerners, our neglect of malaria in favour of diseases which are more profitable or more likely to affect us may be about to turn around and bite us (pun intended).
Plague

Weaponisation is always a good indicator that a pathogen is scary. Plague is a highly infectious disease caused by the bacterium Yersinia pestis. Without treatment it has a high fatality rate. What makes plague particularly scary is the wide range of transmission routes. It is transmitted through airborne droplets; direct contact; indirect contact (e.g. with a contaminated surface); droplets from coughs or sneezes; contaminated food or water; faeces; and it is also transmitted by infected animals such as rats or fleas. Just about the only one missing from the list is sex, but I think that is because we can safely assume that if you get close enough to someone with plague to have sex with them, you are going to catch it.
Plague has a long history as a biological weapon. In ancient China, there are accounts of infected horse and cow carcasses being used to contaminate enemy water supplies. In medieval siege warfare, infected animal carcasses and even human corpses would be catapulted into enemy cities to infect the inhabitants. Some researchers speculate that this is how the Black Death first began to spread through Europe.
More recently, the Japanese used plague as a bioweapon in World War 2. The notorious Unit 731 developed bombs containing infected mice and fleas and used them against the Chinese in the city of Changde, contaminating the city and a wide area around it. They also carried out hideous experiments on prisoners to test the effectiveness of these weapons.
After WW2, both the US and USSR developed biological weapons based on plague, including strains which had been genetically engineered to create antibiotic resistance, and strains which had been combined with other bacteria such as diphtheria. Following the break-up of the USSR, it is possible that there are stocks of bio-weapons that are unaccounted for, and that could potentially fall into the wrong hands.
Still, shouldn’t be a problem because there’s a vaccine, and plague can be treated with antibiotics, right? Wrong. People are not routinely immunised against plague, and if it were used in, for example, bio-terrorism or a biological warfare attack on a civilian population, it would be too late for vaccination. Antibiotics may prove useless against genetically engineered strains. And, resistant strains have occurred naturally; for example, there have been outbreaks of a resistant strain in Madagascar as recently as 2017.
Anthrax

Anthrax is another bacterial infection, caused by Bacillus anthracis. It can affect the skin, respiratory system or gastro-intestinal (GI) tract. Cutaneous (skin) anthrax is rarely fatal if treated, but is unpleasant and debilitating. Untreated, it causes death from septicaemia in about 20% of cases. Respiratory anthrax has a mortality rate of about 45% with treatment; untreated it is almost invariably fatal. GI anthrax is rare but has a mortality rate of 20-65%, depending on how quickly it is diagnosed and treated.
Anthrax can also affect cattle and sheep and is generally fatal because once symptoms appear, death is very quick, typically 2-3 hours. This means that both treatment and quarantine may be difficult. Infection can spread to other animals and humans through contact with infected animals or their remains.
The really scary thing about anthrax is that the bacteria can form spores, going into a sort of dormant state. These spores can survive for very long periods outside a host, for example in soil. In 1942, Gruinard Island off the coast of Scotland was used in a biological warfare trial involving anthrax bombs. Access to the island was forbidden until 1990, when it was re-opened to the public after a decontamination operation that had taken 4 years.
Anthrax was used as a biological weapon by Germany in WW1 and Japan in WW2 (Unit 731 again). In 1944 the British manufactured about five million animal feed pellets contaminated with anthrax; the plan was to drop them over Germany, infecting millions of cattle which would then infect humans. During the Cold War, the US and USSR continued to develop anthrax weapons.
The other really scary thing about anthrax is that the spores are relatively easy to cultivate; in theory, anyone with a moderate amount of microbiology and some fairly basic equipment can do it. This makes it attractive to bioterrorists as well as the military.
Smallpox

Smallpox is a highly infectious disease that is spread through airborne droplets, direct contact with an infected person or contact with a contaminated object. Before Edward Jenner’s discovery of vaccination, it was one of the leading killers in Europe. Those who survive smallpox are often left disfigured by scars or in some cases are blinded. It’s been used as a biological weapon since the 18th century; most recently, the USSR stockpiled tonnes of weaponised smallpox during the Cold War. And, of course, during WW2, our Japanese friends Unit 731 experimented with it extensively.
In 1980, the World Health Assembly officially declared that smallpox had been globally eradicated, thanks to a comprehensive world-wide vaccination program. Only two known samples remain, stored under the strictest security at the CDC in America and a high security bio-research facility in Russia. So, what’s the problem?
The problem is that word ‘known’. Actually, since 1980, other samples have turned up. For example, in 2014, six vials of smallpox dated 1954 were found in a cold storage facility in a Federal Drug Administration laboratory in the USA. They were transferred to the CDC and destroyed, but not before tests showed that the virus was still viable. Other samples may be hidden away in countries that would be less scrupulous. For example, can we really be certain that all virus stocks held in the former USSR have been accounted for?
Another problem is that even if all remaining samples are eradicated, smallpox could still be recreated. This was demonstrated in 2017 when Canadian researchers recreated the extinct horse pox virus, which is closely related to smallpox. Worryingly, they also demonstrated that this could be done by scientists without specialised knowledge, using basic lab equipment and at a relatively low cost; meaning that in theory at least, it could be done by bioterrorists or rogue nations.
Tuberculosis

Tuberculosis (TB) is an infectious disease caused by the bacterium Mycobacterium tuberculosis. It most commonly affects the lungs, attacking and destroying lung tissue. Scarring may occur where damaged lung tissue has healed. In some cases, other organs such as the brain or bones are affected.
It is thought that approximately 25% of the world’s population are infected with the TB bacterium. In 90% of cases, the infection is latent; the remaining 10% have active TB and are able to spread the infection through airborne droplets. Latent TB may become active due to immunosuppression, aging, malnutrition and certain diseases such as diabetes. At the present time, the biggest cause of latent TB becoming active is HIV.
M. tuberculosis is particularly dangerous because of its ability to evade the immune system. It is enclosed in a thick, waxy capsule which protects it from the chemicals that are used to destroy bacteria during phagocytosis. A M. tuberculosis bacterium that is engulfed by a macrophage will not be destroyed; in fact, it will reproduce inside the macrophage. This also prevents antigen presentation, so that the adaptive immune system is not activated.
The same waxy capsule makes M. tuberculosis very difficult to kill with antibiotics. Many antibiotics work by destroying bacterial cell walls; the waxy coating of M. tuberculosis is highly resistant to this. TB must be treated using specialised antibiotics; for example, ones which inhibit the synthesis of the waxy coating.
The rate at which M. tuberculosis develops antibiotic resistance is increasing, with a growing number of strains that are resistant to multiple drugs. Depending on the drugs used, treatment of TB with antibiotics takes 3-9 months, during which time the patient will usually be taking a combination of two or more antibiotics. Some patients stop taking medication before the infection has been eliminated, meaning that their treatable TB is at risk of becoming resistant. In poorer countries, the sale of sub-standard or counterfeit antibiotics also contributes to resistance.
Prior to 2005, all secondary school pupils in the UK were offered the BCG vaccine, which protects against TB. In 2005 this practice was discontinued due to the very low rates of TB in the UK. It was replaced with a targeted vaccination program in which the vaccine was offered only to those considered to be at risk of coming into contact with active TB. The effectiveness of the vaccine is variable. Studies have found that in the UK, the vaccine prevents TB infection in 60-80% of people. The duration of protection from the vaccine is also highly variable, meaning that some people who were vaccinated in childhood may no longer be protected. Outbreaks of TB in the UK are on the increase. This is due partly to immigration from countries where there are high rates of TB, and also due to the fact that more people with latent TB are developing active TB as a result of HIV.
So why does TB make the list? It’s difficult for the immune system to fight, and the vaccine may not offer effective protection. TB is developing antibiotic resistance at a worrying rate. There is a real risk that the rate of development of resistance will increase to a point where drug development cannot keep up, and strains emerge which are untreatable.
Influenza

They say familiarity breeds contempt, and nowhere is this truer than the humble flu virus. Typically, seasonal flu will cause an illness which, in healthy adults, is unpleasant but rarely fatal. However, even ‘normal’ seasonal flu can cause life-threatening complications in vulnerable people such as young children, the elderly, the immunosuppressed and those with pre-existing medical conditions.
Flu viruses mutate rapidly. However, simple mutation leads to relatively minor antigenic variation, so that individuals immune to the old strain may still have some immunity to the new one, which limits the spread of normal seasonal flu. A bigger problem is that influenza viruses can also undergo re-assortment; this occurs when different strains of the virus mix their genetic material and recombine it, resulting in a completely new virus. It happens when two different strains of virus infect the same host and leads to major genetic shifts and completely new antigens. When this happens, there is zero immunity in the population and available vaccines will not be effective; there is no herd immunity and this leads to a pandemic. Examples of this are the Spanish Flu pandemic of 1918-19 and the H1N1 Swine Flu pandemic in 2009.
The new viruses that result from re-assortment are not necessarily any more virulent than existing strains; the higher death rate from pandemic flu is because there is no vaccine or herd immunity, so vulnerable members of the population are unprotected. The Spanish Flu of 1918-19, which killed more people than WW1, was unusual because the mortality rate was highest among young, healthy adults. Recent research suggests that the virus triggered a cytokine storm. This is an abnormal immune response which caused activated immune cells to flood the lungs, leading to inflammation and build-up of fluid. Medical professionals at the time called this ‘dripping lung’. Patients either drowned in their own secretions or fell victim to secondary pneumonia. Ironically, the better your immune system, the more likely you were to suffer a cytokine storm, which is why the pandemic killed so many healthy adults.
More recent flu pandemics have not had the same mortality rate, partly because those viruses did not trigger a cytokine storm, and also because modern antibiotics were available to treat secondary bacterial infections. New anti-inflammatory drugs to treat cytokine storms are being researched; let’s hope they come into clinical use before a Spanish Flu type virus occurs.
Foot and mouth disease

You may be surprised to see that two of the pathogens that make this list are ones which do not even infect humans. Foot and mouth disease (FMD) is a highly infectious virus that affects cloven-hoofed animals such as cattle, sheep, pigs and goats. Although it is rarely fatal, it is extremely debilitating to infected animals and causes significant suffering. They suffer lameness due to blisters on the feet, and are unable to eat due to blisters in the mouth. This leads to severe weight loss, and animals take several months to recover. Milk production in females and fertility in males is also severely affected. Humans cannot catch FMD; when people claim to have had FMD, what they have actually had is hand, foot and mouth disease. This is a mild viral illness that typically lasts about a week.
FMD is highly infectious and can spread through direct contact between infected animals, or by indirect contact with contaminated items; for example, farm machinery or farmworkers’ boots and clothing. Meat products from infected animals can also carry the virus and it can even survive pasteurisation of milk. FMD has an incubation period of 1-12 days, during which the infected animal can pass the virus on to others. Because of the potential for rapid spread of infection, once it has been detected on a farm, all susceptible livestock must be culled and the carcasses burned or buried at an approved site.
FMD cannot infect humans, so why include it in my top ten? Quite simply because it has the potential to literally cripple a country, its infrastructure and its economy. The last major outbreak of FMD in the UK was in 2001 and lasted 9 months. Over 6 million cows and sheep were culled to try and halt the spread of the disease. Severe restrictions on the movement of animals meant that even farmers whose farms were not infected suffered significant financial losses. The tourism industry was also badly affected, with the number of overseas visitors to the UK dropping by 10%. All public rights of way were closed, and some major events were cancelled. It is estimated that the economic loss to agriculture was about £3.1 billion, with a loss of between £2.7 – 3.2 billion to other sectors of the economy such as tourism. The potential of FMD to damage economies and divert resources into combatting it could make it a potentially attractive agent for biological warfare or bioterrorism.
Canine distemper

Canine distemper (CD) is an infectious disease that can infect a range of carnivores including canines (e.g. dogs, wolves, and foxes), mustelids (e.g. ferrets, mink and otters), big cats, seals, and skunks. Recently it has begun to cross into non-carnivores including Asian elephants, pandas and some species of primate. CD affects the respiratory and central nervous systems, and has a very high fatality rate. It is transmitted by droplets in the air or contaminated objects. The virus can survive for a fairly long time outside a host, for example on fur that has been shed by infected animals.
The CD vaccine is highly effective. CD does not affect humans, and does not have the potential to affect the economy the way FMD does. So why does CD scare me? Basically because of its remarkable ability to cross between different species. Within a relatively short time, CD has jumped from canines and mustelids into other carnivores, and then into non-carnivores. Most worrying of all is its recent jump into primates. Laboratory experiments have demonstrated that the strain which affects monkeys has the potential to interact with proteins on the cell membranes of human cells, meaning that in theory at least, CD could at some point cross into humans. The human population is mostly unprotected (immunity to measles does give some crossover protection against CD) and it would take time to develop an effective human vaccine. Most of the UK’s domestic dog population is vaccinated, but vaccination is not compulsory. Uptake of the vaccine among ferret owners is variable, and some vulnerable domestic pets such as skunks cannot currently be vaccinated. There is a huge reservoir of disease in the wild animal population, meaning that if the virus did become capable of infecting humans, the risk of a major outbreak would be significant, potentially resulting in a large number of deaths.
March 2021: Ironically, the COVID pandemic may actually result in a significant reduction in the risk of CD crossing into humans. In 2020, COVID-19 was discovered in mink on intensive fur farms in Scandinavia, resulting in a large-scale cull. The overcrowding in such farms provides ideal conditions for a pathogen to jump species: if COVID could jump from humans into mink, there’s a definite possibility of CD going the other way. If COVID means the end of intensive mink farming, then a significant risk will have been removed, as well as a major animal welfare issue.
COVID-19
Did not make the original list! I wrote the original in January 2020, when it still looked as though the virus might be containable. A year later, we were in lockdown #3, the UK death toll had passed 100,000, and new strains were emerging which became ever more infections. COVID-19 really is the gift that keeps on giving!
Now it’s February 2022 and the dominant strain is the omicron variant, which is highly infectious but causes only mild illness in the majority of people. This is likely to be due to the successful rollout of vaccines; but also that COVID-19 is following a well known evolutionary pattern by becoming more infectious but causing less severe disease. I will post more on this soon.

There is one good thing that has come out of the pandemic, and that is that immunology, and particularly vaccine science, has taken a huge leap forward. RNA vaccines have been in development for a number of years, but 12 months ago, not a single one had made it into clinical usage. Now, we have two RNA vaccines (Pfizer and Oxford/ AstraZeneca) being rolled out on a large scale, with others expected to gain regulatory approval in the next few weeks. It is my belief that the pandemic has advanced vaccine science in the same way that WW1 advanced radiography and blood transfusions; and WW2 advanced the use of antibiotics.
Ebola – the one that didn’t make it.
When I wrote the original blog post, a few people asked me why Ebola didn’t make the list of my top 10. It still doesn’t, and here’s why.
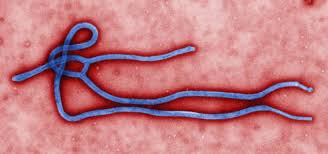
Ebola is one of a group of viruses called filoviruses. These have filament-like structures which coil to form a characteristic ‘shepherd’s crook’ shape. Like all viruses, Ebola invades cells and uses their organelles to reproduce. Ebola reproduces rapidly and efficiently. It triggers the release of chemicals that cause healthy cells to die; it also causes cell death by using up resources such as proteins at such a rapid rate that the cell is no longer able to maintain membranes and other structures.
Ebola causes damage and death to the endothelial cells that line blood vessels, leading to vascular instability – blood vessels literally disintegrate. At the same time it damages liver cells, impairing the clotting process. This results in massive and often fatal internal bleeding. It is able to evade the innate immune system by blocking the production of interferons. These are chemicals that are normally produced by cells which are infected with viruses; they signal natural killer cells (NKCs) to destroy the infected cell. Blocking the release of interferons allows Ebola to reproduce unchecked. The average death rate from Ebola is about 50%, but it can be as high as 90% depending on the strain. Death usually occurs as a result of hypovolemic shock – low blood pressure due to blood and fluid loss.
Remember when I said earlier that weaponisation is a good indication of how scary a pathogen is. Ebola is a devastating disease, highly infectious and with a high mortality rate. It’s a particularly gruesome pathogen as well – sufferers can literally bleed to death internally. This generates fear in the wider population; on the face of it, Ebola has all the makings of a weapon that would induce mass panic and terror as well as widespread death. But, Ebola has never been weaponised. And the reasons it has never been weaponised are the same as the reasons why it didn’t make my original ten.
Put simply, Ebola is too efficient for its own good. It reproduces so rapidly that it quickly destroys the cells it infects, killing its host in the process. The most deadly viruses are the ones that keep their hosts alive for long enough to infect as many others as possible. Even without intervention, Ebola outbreaks burn out relatively quickly.

There are two other reasons Ebola still doesn’t make the top 10: transmission and survival outside a host. Ebola can only be transmitted through direct contact with the bodily fluids of an infected person: blood, saliva, vomit, semen etc. This means that use of PPE is highly effective in bringing an outbreak under control. In recent years, the importance of safe burial practices has also been recognised. This involves burying the dead as soon as possible; sealing the body inside leak-proof body bags; and ensuring that those handling the dead use PPE and hygiene measures effectively.
The other problem Ebola has is that it can only survive for very short periods outside a host, and is very easily destroyed by simple agents such as soap, bleach or detergent. The failure to weaponise Ebola (and trust me, several nations have tried!) is also down to its poor survival. You couldn’t put Ebola in a bomb, for example, because the detonation of the bomb would kill it off. A spray would also be of limited effectiveness, because the virus would only be viable for a very short period of time.
