First of all, hi there to all my readers! I’m sorry I haven’t written anything in a while. Things have been intense with the day job – any teachers reading this will know that working from home and delivering remote learning is actually a lot more labour intensive than face-to-face teaching. Like so many other people, I’ve also been finding social distancing tough. I’ve been asked how I cope with it, and the simple answer is, because I know that I have to. In this article I will be looking at the 1918-19 Spanish Influenza pandemic, and explaining the lessons we can learn from it about social distancing.
It’s inevitable that parallels will be drawn between the situation now, and the Spanish Flu pandemic. This time 100 years ago, the world was reeling from a devastating global pandemic that had killed more people than the preceding four years of war.

The origins of Spanish flu have been hotly debated. There is speculation that the virus originated in China, and was brought to Europe by Chinese labourers working for the British and French armies – a theory that has been seized upon by conspiracy theorists looking for evidence of sinister Chinese involvement in the current pandemic.
Those studying Spanish flu, particularly epidemiologists, have a wealth of data to work with. It was the first global pandemic to occur in an age where there was good record keeping in both military and civillian hospitals.

Detailed studies of records kept by the US Army have actually narrowed down the origin of the disease to the state of Kansas, and the US Army training camp at Fort Riley. The evidence strongly supports the theory that the disease jumped directly from birds into humans, with ‘patient zero’ being a farm worker from a poultry farm who caught the disease just before enlisting in the US Army.
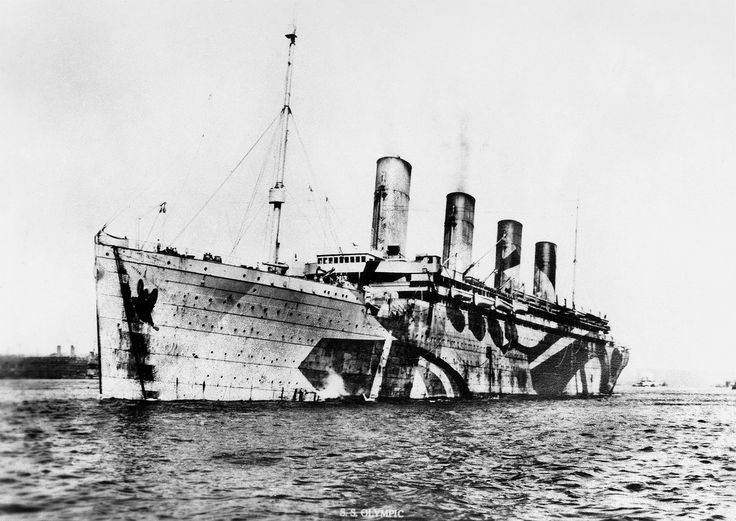
Wartime conditions were almost ideal for spreading the virus. After the first cases were reported, the illness spread rapidly through Fort Riley; movement of troops ensured that it spread rapidly to other camps and into the civilian population. Troops with the illness were sent overseas to fight, meaning that the disease very quickly spread to England and to continental Europe. It is ironic that the entry of the USA into the war, which was instrumental in bringing it to an end, also ensured that the Spanish flu outbreak became a pandemic.

I won’t dwell here on the disease itself and its effects. If you want to know more, I thoroughly recommend Lyn McDonald’s book ‘The Roses of No Man’s Land’ which contains harrowing first-hand accounts from doctors, nurses and others, of the effects of the illness in crowded military hospitals, camps and troopships.
What I find interesting, and highly relevant, about the Spanish flu pandemic, are the lessons we can learn about social distancing. Wartime conditions meant that social distancing simply wasn’t possible – in fact, the opposite was the case with people crammed together in hospitals, training camps, troopships and, of course, the trenches themselves.

Another, more pernicious factor that contributed to the spread of the disease was lack of public information. Basically, the public were not told about the illness for fear that it would damage morale in the critical final months of the First World War. People who could have practiced social distancing didn’t, for the simple reason that they did not realise there was any need to. The pandemic got its name because in neutral Spain, there were no restrictions on the press; they were even free to report when King Alfonso XIII became seriously ill. This led to a misconception that Spain was particularly hard hit.
Not only was social distancing not practised, the British government actually discouraged authorities from putting measures in place to limit the spread of the infection. Medical officers in large cities were discouraged from closing schools, churches, cinemas, theatres, dance-halls etc.; again, out of fears that this would damage morale.
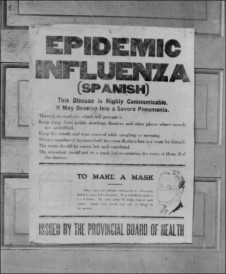
One man who went against this was Dr James Niven, medical officer for Manchester. Against direct advice from the government, he closed schools and entertainment venues, and distributed posters and leaflets giving information about the illness and advice on how to protect against infection (mainly, ‘wash your hands’ – sound familiar?). Niven insisted on quarantine for those who were sick, gave regular interviews to the Manchester Guardian to keep the public informed, and took measures to deal with delays in funerals.
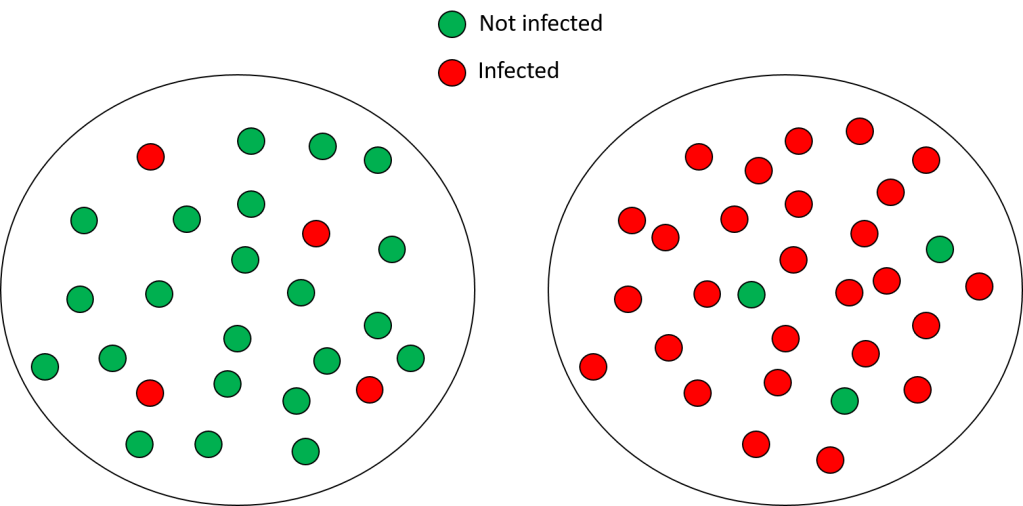
As a result, the rate of infection in Manchester was lower than in other large cities with similar population densities. The death rate among those infected was also lower, because medical services were now overwhelmed as they were elsewhere. High tech devices such as ventilators were not available in those days, but high quality medical care, particularly intensive nursing, could make all the difference between surviving or dying from the illness.
I’ve no doubt that during the Spanish flu pandemic, there were those living in Manchester who resented the restrictions. Why were their cinemas closed when those in other cities remained open? No doubt, too, there were those who regarded Niven’s information campaign as exaggerated or scare-mongering. I also am in no doubt that if I went back in time to 1918 and had to live in a large city in the UK, I would choose Manchester with its social distancing.
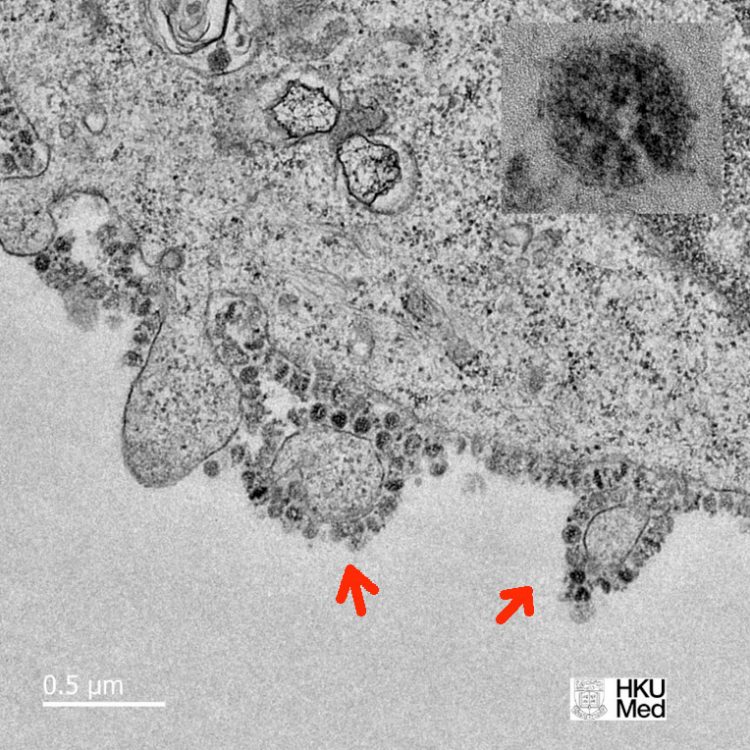
In my next post I will be discussing the differences between oxygen therapy, continuous positive air pressure (CPAP) and ventilation; and the role they all have to play in helping people survive COVID-19. Stay well and safe, everyone.