In this post I will try to answer three questions that are related to each other. How do new viruses evolve, how do viruses spread from animals to humans, and can viruses change when they start to spread.
In my last post, I talked about how viruses contain a strand of DNA or RNA which holds all the information needed to make new copies of the virus. When a virus reproduces, part of the process is making a new copy of either the RNA or the DNA.
DNA, which stores information.
If you’ve ever had to copy something out, you’ll know that from time-to-time, you make a mistake. The same thing can happen when new copies of the virus’ DNA or RNA are made. These mistakes are called replication errors. The altered DNA or RNA can still be used to make new viruses, but they will be different – this is called a mutation.
Replication errors do not produce completely new viruses. Instead, they produce new versions of the original virus – these are called strains. Viruses which store their information as RNA have more replication errors than those with DNA. There are two reasons for this. RNA is designed to store information for shorter periods of time, so it is less stable than DNA. Also, remember, the virus is using the organelles of a cell to copy itself. The organelles in a cell are designed to copy DNA, not RNA. They have all sorts of safety mechanisms to prevent replication errors when copying DNA, but these won’t work for RNA. The common cold is caused by RNA viruses, this is why there are so many different strains of it.
Flu is also caused by an RNA virus. As well as replication errors, flu viruses can do something called re-assortment. Basically, if two different strains of flu infect the same person or animal, they can mix their RNA together and then recombining it, giving a new strain which is very different to the old ones. The most recent example of this was swine flu in 2009.
So, what about coronavirus COVID-19? It’s an RNA virus, so whenever it reproduces there may be replication errors. Most replication errors actually cause changes that make viruses weaker, and these strains die out very quickly. Very occasionally a replication error will give a new strain that survives.
So, is COVID-19 a completely new virus? The answer is no, and this relates to the second question, which is about how viruses spread from animals into humans. If you’ve read my post about how viruses work, you’ll know that they invade cells and take them over in order to make new viruses. The first step in this is to stick onto the surface of a cell.
Spikes on the virus must match exactly with receptors on a cell.
The envelope of a virus is covered in proteins, called spikes, which it uses to attach itself to a cell. These proteins will attach to proteins on the cell surface called receptors. For this to happen, the shape of the spike has to match up with the receptor – like a key fitting into a lock, or two jigsaw puzzle pieces fitting together. If the key, or the puzzle piece, is even slightly the wrong shape, it won’t fit.
There are a lot of viruses that affect animals but which humans can’t catch – this is because the spikes are the wrong shape to attach to human cells. Every so often though, a mutation will occur which alters the shape of the spikes, so that they can attach to human cells. Humans can now catch the new strain of the virus.
COVID-19 spread from animals when a mutation changed the shape of the spikes so they now match receptors on human cells.
So, how did this happen with COVID-19? Viruses are more likely to cross from animals into humans if there is a lot of contact between them. Wuhan, in China, where the virus was first seen, has a large market where live animals are sold. The city is also very overcrowded, so it’s easy for viruses to spread. Scientists think that the virus spread to humans from animals being sold in the market. They aren’t sure which animal, but coronaviruses are common in bats, and in an animal called a pangolin – both of those were on sale in Wuhan.
The final question is, do viruses change when they start to spread? The answer is, yes. The more a virus spreads, the more it reproduces, so the more opportunity for replication errors. With a virus like flu, there is also more chance of the same person or animal being infected by two different strains, leading to re-assortment. So, how will COVID-19 change as it spreads? The answer is that any changes are likely to be very small, because they will be due to replication errors – coronaviruses can’t undergo re-assortment like flu viruses do. Changes are likely to be very minor and will not alter how the virus affects humans. Scientists working on a vaccine will also be making sure that it will still work if there are changes to the virus.
I hope you have found that useful! In my next post, I will be looking at how scientists study new viruses and find out how they work.
This is the first in a series of posts where I hope to answer some questions I’ve been asked about coronavirus by children. The first question I will try and answer is: what is a virus?
To understand viruses, we first need to understand a few things about cells. Your body is made up of millions of cells, which are the smallest form of life.
Human cells from inside the cheek, seen under a microscope.
Cells are tiny – they are about 100 millionths of a metre in diameter. You can see them under a light microscope – if you are in Year 7 or 8 you have probably done this at school.
There are lots of different types of cells, and some look very different to the picture on the right. But there are certain structures, called organelles, that nearly all cells have, and these are shown in the diagram below.
The cell membrane is around the outside of the cell and controls what goes in and out of the cell. The inside of the cell is called the cytoplasm. Mitochondria are the cell’s power source – they take glucose (from our food) and react it with oxygen (from the lungs) to provide the energy the cell needs. Ribosomes are the cell’s factories – they make all the various substances that the cell needs. The nucleus contains the instructions the cell needs to function, stored on a molecule called DNA. More about that in another post.
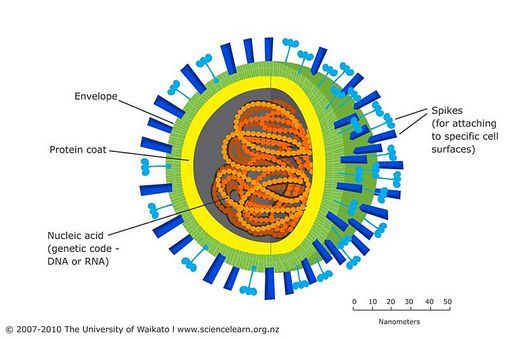
The structure of a virus is very different to a cell. To start with, they are much, much smaller. Viruses are about 1000 times smaller than human cells. The goal of a virus is simply to reproduce – to make as many copies of itself as it possibly can. That is literally all they exist to do. The structure of a virus is a lot simpler than that of a cell, as shown in the diagram below:
Structure of a virus. A nanometre is one billionth of a metre
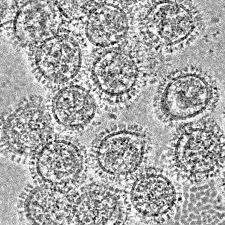
Influenza viruses seen with an electron microscope. You can clearly see the spikes on the envelopes of each virus.
As with cells, there are lots of types of virus and some look different to the one in the diagram. But they all have certain structures in common. All viruses have a protective capsule, called the envelope, which protects the contents. On the surface of the virus there are protein molecules sticking out – these are called spikes, and help the virus attach itself to a cell.
Inside the envelope is a strand of either DNA or RNA. These are molecules which carry all the information the virus needs to make copies of itself. Basically, the DNA or RNA is an instruction manual for making more viruses.
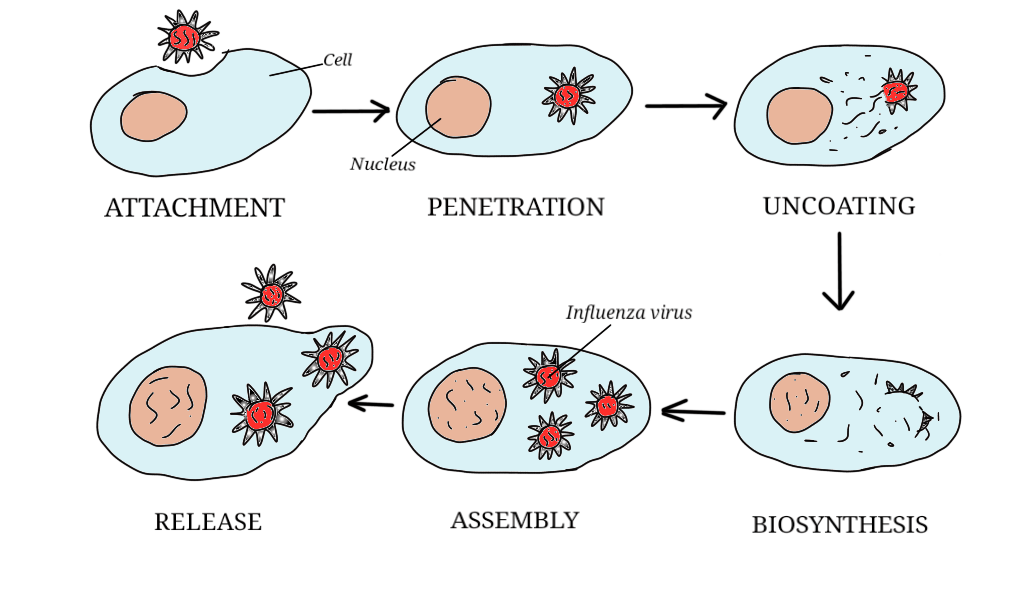
But, viruses have a problem. They don’t have any organelles, and they need them in order to reproduce. They need a nucleus to process the DNA or RNA (a bit like reading the instructions). They need mitochondria to provide energy, and they need ribosomes to make and assemble the new viruses. They solve the problem by taking getting inside a cell (called the host), taking over its organelles and using them to make new viruses. Here’s how its done:
Attachment. The spikes on the surface of the virus stick to the surface of the cell. Have you ever been for a walk in long grass in summer, and come back with those spiky seeds stuck to your clothes? It’s a bit like that.
Penetration. Once the virus has attached itself to the cell surface, it can penetrate the cell membrane and get inside.
Uncoating. The envelope of the virus breaks apart, releasing the contents into the cell.
Biosynthesis. Synthesis is basically a scientific word for making something. Biosynthesis is when the virus takes over the cell’s organelles and uses them to make everything needed for a new virus.
Assembly. The virus uses the cell’s organelles to put the new viruses together.
Release. The virus destroys the cell membrane so that the cell bursts open and releases the new viruses. They then go on to infect other cells.
So, how do viruses make us ill? Partly by the damage they do to our cells, but also as a result of the things our body does to fight them off. More of that in a later post.
I really hope you have found this post useful. Coming up tomorrow: how viruses change, and how viruses move from animals into humans. If you have any questions you’d like me to try and answer, please send them to me by comment, email or Facebook!
I’ve had a request from a friend whose 9-year old daughter has a lot of questions about COVID-19, and it’s made me realise there is a lack of good quality, child-friendly information out there. I passionately believe that knowledge and understanding are important for all age groups, and that children deserve to have their questions answered and their concerns addressed. So, over the next few days I will attempt to answer her questions, and any others people have. As always, my aim is to provide information that is accessible but not patronising! The questions I will be attempting to answer are:
What is a virus?
How do new viruses evolve?
How do viruses spread from animals to humans?
How do scientists study new viruses?
Can viruses change when they start to spread?
How does washing your hands affect viruses?
If your child has any questions that you’d like me to try and answer, please get in touch and I will do my best! I am also looking at possibly holding an online question and answer session for children, if that is something that would be an interest.
This post is a bit of a departure from previous posts on this blog. It’s the first of a series of posts in which I will be exploring the lives, and contributions to science, of a variety of different people. In particular, I will be writing about scientists who are perhaps not as well recognised as they should be; who are controversial; whose demise occurred before they could realise their potential; or who were just downright quirky. As today is International Women’s Day, I will talk about a woman whose contribution to science was immense, but has been eclipsed by that of her mother.
Think of radioactivity and one name will almost certainly spring to mind: that of Marie Skłodowska Curie. Marie Curie is famous as the discoverer of radium and polonium. She was not only the first woman to win a Nobel Prize, she remains the only person of any gender to have won two for different disciplines: physics and chemistry. This post will explore the life of another female scientist who is less well known, but just as deserving of recognition: Marie’s older daughter, Irène Joliot-Curie. Not only did Irène make some very significant scientific discoveries, she was politically active, being both a pacifist and feminist.
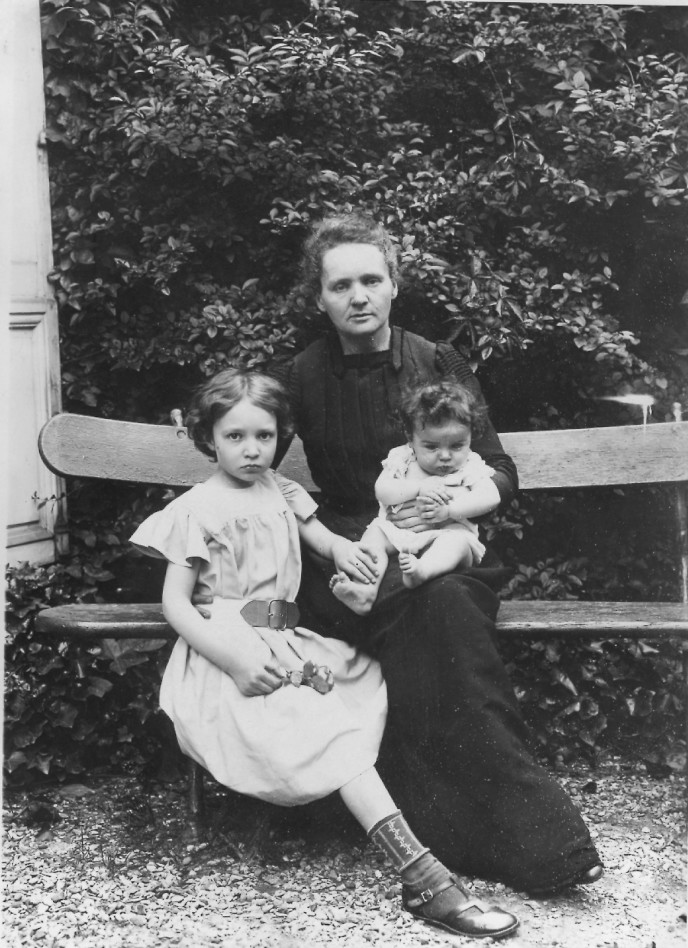
Marie Curie with Irène and Ève in 1905
Irène was born in Paris in 1897 and her earliest years were not always easy. Her parents Marie and Pierre were absorbed in their work, putting in long hours on the research that would win them the 1903 Nobel Prize for Physics alongside Henri Becquerel. In these early years, Irène, and later her sister Ève, were largely raised by their paternal grandfather, retired doctor Eugene Curie. He taught Irène to love nature and the arts, particularly poetry, and also got her interested in radical politics. Marie herself acknowledged the difficulty of balancing work and family, writing that,
“I have frequently been questioned, especially by women, of how I could reconcile family life with a scientific career. Well, it has not been easy.”
By the time Irène was born, the health of her father, Pierre Curie, was declining rapidly, almost certainly due to his exposure to large doses of radiation. He was killed in 1906 when he was hit by a horse-drawn vehicle in a Paris street. This has been attributed to his having been distracted by thinking about his work, but it is highly probable that radiation exposure contributed. Cognitive impairment and fatigue are common in conditions associated with high radiation exposure, such as leukaemia and aplastic anaemia.
Marie was devastated by Pierre’s death, and struggled more than ever to balance her scientific work with the demands of bringing up two young children (Ève was only 16 months old when Pierre died). However, after Pierre’s death, Marie made the decision to spend more time with her children. She withdrew Irène from public school to educate her in a ‘co-operative’ organised by a group of 6 professors, including Marie, who taught each other’s children in their areas of expertise. In this way, Marie was able to nurture Irène’s love of, and obvious talent for, mathematics and science, and the two grew increasingly close. Marie was a demanding teacher though; even on holiday, Irène was expected to study for a certain amount of time each day.
The education that Irène received at the co-operative was not restricted to mathematics and science. On the contrary, it was wide ranging and included arts and languages; there was also considerable emphasis on self-expression and play. It is tempting to believe that Irène was forced into a life of science by her mother, but this was not the case, as is shown by her sister Ève. Ève did not have a scientific bent but preferred the humanities, and Marie supported her wholeheartedly. Ève would go on to have a distinguished career as a journalist and political activist, eventually living to the age of 102. Ève was just as close to her mother as Irène, and both sisters together nursed Marie through her final illness.
For the final two years of high school, Irène returned to a more conventional education, studying at the College Sevigne in Paris. In 1914, she took up a place at the Sorbonne to study mathematics and physics. However, like many young people at the time, her education was to be interrupted by the outbreak of World War 1 in August 1914.
Irène and Marie Curie in an X-ray unit at a hospital in Belgium, 1915
From the very outset of the war, Marie Curie recognised a need for radiography services to be provided as close to the Front as possible, to aid surgeons in operating quickly on wounded soldiers. Her first mobile radiography unit was operational in 1914, and she was appointed director of radiology services for the Red Cross. Irène assisted her mother when she could, taking a nursing course alongside her other studies. In 1916, Irène left the Sorbonne in order to work alongside Marie as a full time nurse-radiographer.
Within a few months, 19-year-old Irène was in sole charge of a battlefield radiography centre in Belgium. She taught herself how to maintain and repair the equipment, and she taught doctors how to locate bullets and shrapnel using X-rays. Irène worked in a number of locations, including Ypres and Amiens. Marie and Irène’s work in developing the use of medical X-rays saved the lives of many soldiers, and also helped to significantly advance the uses of medical radiography.
Irène descending from a mobile X-ray car. These were known to French troops as ‘Petits Curies’
Following the end of the war, Irène returned to the Sorbonne and completed her degree in maths and physics, before moving to the Radium Institute to work once again as her mother’s assistant. In 1925 she completed her doctoral thesis on the radioactive properties of the element polonium.
Irène was an expert in the highly specialised and precise techniques required to study radiation. So much so that in 1924 she was asked by Marie to train a newly appointed researcher at the Institute: chemical engineer Frederic Joliot. Irène and Frederic were married in 1926 and took the surname Joliot-Curie. Irène and Frederic combined their research efforts, just as Marie and Pierre Curie had before them, specialising in the study of atomic structure. Their early work identified the existence of both the neutron and the positron; however, they did not recognise the significance of their results, so the discoveries of both are credited to other scientists.
Irène at the Radium Institute in 1922
Irène and Frederic struggled to get some of their early work accepted by the scientific community. They carried out experiments involving bombarding aluminium with alpha radiation, and their results showed that a proton can change into a neutron by emitting a positron (similar to an electron, but with a positive instead of a negative electrical charge). However, when they tried to present their findings to the wider scientific community, they came in for extensive criticism.
Irène and Frederic at work
It was this early work that led to the discovery that would gain them recognition, and a Nobel Prize. Continuing their experiments with aluminium and alpha particles, they found that if a non-radioactive element is irradiated alpha particles, it is possible to turn it into a different, radioactive one.
How does this work? An alpha particle consists of two protons and two neutrons – it’s basically a helium nucleus without the electrons. If an alpha particle collides with an atomic nucleus with the right amount of energy, it will combine with the nucleus. Aluminium has 13 protons and 14 neutrons. When an alpha particle collides with an aluminium nucleus, two protons and one neutron combine with the nucleus, giving 15 protons and 15 neutrons. If you change the number of protons in a nucleus, you get a different element – in this case, phosphorous. Irène and Frederic had finally achieved what the medieval alchemists never could: changing one element into another.
More importantly, the phosphorous they made by this method was radioactive. The reason for this is that phosphorous normally has 16 neutrons, and the phosphorous made by Irène and Frederic only had 15. Atoms with the same number of protons but different numbers of neutrons are called isotopes, and the only stable isotope of phosphorous has 16 neutrons. The isotope made by Irène and Frederic quickly decayed into a more stable form, changing into the element silicon and emitting radiation in the form of beta particles. Using the same method, Irène and Frederic were able to create several other artificial radioactive isotopes.
The importance of the discovery of artificial radioactivity cannot be over-emphasised. The use of radioactive isotopes in medicine was growing rapidly, and Irène and Frederic’s discovery meant that radioactive materials could be created cheaply and in large quantities. Many of the radioactive isotopes used in modern medicine are manufactured using their method, although usually a beam of neutrons is used rather than alpha particles. For example, cobalt-60, which is used in radiotherapy to treat cancer, is made by bombarding stable cobalt-59 with neutrons.
Irène and Frederic in 1935, shortly before being awarded the Nobel Prize for Chemistry
In 1935, Irène and Frederic were awarded the Nobel Prize for Chemistry, and finally gained the recognition of the scientific community. Irène was also given a professorship in the faculty of science at the Sorbonne. Over the next few years, she and Frederic led research into the element radium which led in 1938 to the discovery of nuclear fission by a group of German scientists.
Throughout the 1930s, Irène and Frederic were aware of, and concerned by, the growth of fascism; during the Spanish Civil War they were strong supporters of the Republican faction. In the late 1930s they stopped publishing their work due to concerns about its possible military uses. In October 1938, they placed all documents relating to their work in a secure vault at the French Academy of Sciences, where it remained until 1948.
In 1941, Irène contracted tuberculosis and was forced to leave France and go to a sanatorium in Switzerland. Her husband and children remained in France, where Frederic became an active member of the resistance. Despite the danger, Irène made several trips back to France to visit her family, and on several occasions was detained by German guards at the Swiss border. In 1943 Irène returned to France, but it was becoming more and more dangerous. In early 1944, Irène returned to Switzerland, this time taking their two children, Helene and Pierre. They remained there for several months, not knowing whether Frederic, who had stayed behind to continue his work with the resistance, was alive or dead. Eventually, the family were reunited in September 1944 when the liberation of Paris made it safe for Irène and the children to return.
After the war, Irène followed in her mother’s footsteps by being appointed director of the Radium Institute. Irène and Frederic both turned their attention to the use of nuclear fission to generate electricity, becoming respectively the commissioner and director of the newly formed French Atomic Agency Commission. Under their direction, the first French nuclear reactor was created in 1948, and was able to generate five kilowatts of power. A long-lasting legacy of the Joliot-Curies is France’s extensive use of nuclear power, which generates approximately 80% of the country’s electricity.
Irène at the controls of the first French nuclear reactor
Irène was a passionate and active member of the feminist movement, who campaigned throughout her life for women in science to get the recognition they deserve. The French Academy of Sciences would not admit women, and she confronted this chauvinism head-on, writing letter after letter of application. She knew that she would be turned down, but felt it her duty to draw attention to their refusal to admit her because she was a woman. Irène used her position and influence to promote education for women, and she served on the National Committee of the Union of French Women. In 1936, she was appointed to a powerful political position as Undersecretary of State for Scientific Research by the French government – ironic, considering that at the time, women could not vote.
Irène with close family friend and fellow pacifist Albert Einstein on the steps of his home in Princeton, NJ, 1948
Irène was also a devoted pacifist. She knew that the discoveries she and Frederic had made could be put to military use, hence their decision to hide their research at the start of WW2. Her bout of TB in 1941 may have been a blessing in disguise; neither side could try to recruit her for their nuclear weapons programs because she was simply too ill. By contrast, her mother’s close friend Albert Einstein was coerced into signing a letter endorsing the Manhattan Project, which he would regret for the rest of his life. In 1948, Irène was an active member of the French delegation to the World Congress of Intellectuals for Peace, and she continued to campaign for peace throughout her life.
Irène would follow in her mother’s footsteps in one last, tragic way. In the early 1950s her health began to decline and she was diagnosed with leukemia. It is highly likely that this was a result of years of exposure to radiation, just as Marie’s death from aplastic anemia had been. Much of Irène’s work had been with one of the most dangerous radioactive isotopes to human health: polonium-210. Polonium-210 is approximately 250,000 times more toxic than hydrogen cyanide, and was famously used in 2006 to kill Russian dissident Alexander Litvinenko. In 1948, Irène was exposed to polonium-210 when a container of it exploded on her laboratory bench; there is speculation that this caused her eventual death.
Irène underwent surgery and treatment with antibiotics to alleviate her condition, and continued to work as much as she could; in 1955, just months before her death, she was working on plans for new physics labs at the University d’Orsay. Her condition continued to deteriorate and on March 17, 1956, she died in hospital in Paris. Frederic did not outlive her by much; he died in 1958 from liver disease, also linked to radiation exposure. After her death, Irène’s family made sure that her principals of atheism and pacifism were upheld. When the French government asked to hold a national funeral in her honour, they insisted that the religious and military portions be omitted. Perhaps a bigger tribute to them both is that they made the use of radioactive isotopes in medical imaging and radiotherapy both practical and affordable. Who knows how many lives their discoveries have saved?
I was in a large supermarket the other day and out of interest, decided to have a look for hand sanitiser. Sure enough, the shelves were empty. It was the same in my local shop, where a member of staff told me that new stock couldn’t be had ‘for love nor money’. It didn’t bother me though, because what I was actually looking for was soap.
In the last few days, we’ve seen a lot of ministers and health professionals doing their best to persuade us that soap and water is actually better than alcohol-based hand sanitisers for cleaning and sterilising our hands. In this post, I will explain why they are right, using the diagram below which shows the structure of a coronavirus.
All viruses have the same basic structure: a strand of DNA or RNA encased within a protective envelope. There are various proteins on the surface of the envelope, and it may contain enzymes as well as DNA or RNA. It’s the envelope we are concerned with here, because it protects the genetic material. Destroy the envelope and you destroy the virus.
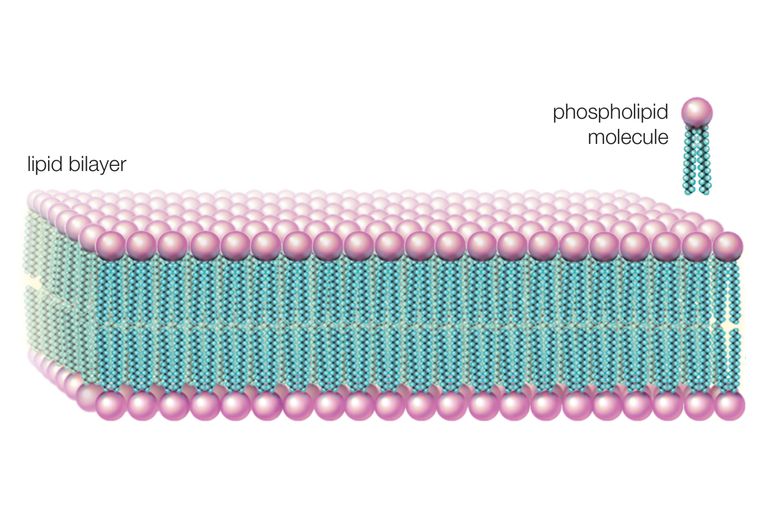
The envelope is made up of molecules called phospholipids. These are a type of fat, and are the same thing that makes up cell membranes. The structure of a phospholipid, shown in the diagram on the right, can be thought of as being a bit like a tadpole. A strange, mutated tadpole that has two tails… The head contains a phosphate ion, and the two tails are made up of fatty acids. The phosphate ion in the head has an electrical charge (it’s polar if we want to get technical), which means it can interact with water – it is hydrophilic. The fatty acid tails are not charged (they are non-polar), which means they cannot interact with water.
In a cell membrane, or the lipid envelope of a virus, phospholipids line up tail to tail, as seen on the left, forming a double layer – the phospholipid bilayer. Disrupting this bilayer will cause the envelope to break down, destroying the virus.
So, why is soap and water better than alcohol-based hand sanitiser? The answer is that soap and water can interact with both parts of the phospholipid. Water is a polar molecule, meaning that it is attracted to anything with an electrical charge. So, water can get in amongst the phosphate heads, causing them to separate. Hydrophobic substances, such as the tails of the phospholipid, do not interact with water, but they do interact with detergents such as soap. So, while the water separates the heads, the soap separates the tails; the envelope breaks up and bingo – no more virus!
Why are alcohol-based hand sanitisers not as good? Basically because they do not include a detergent. Alcohols are polar molecules, meaning that they behave in the same way that water does. Alcohols can interact with the hydrophilic head of a phospholipid, but not with the hydrophobic tail. So, they will destroy the phospholipid envelope of a virus by interacting with the heads, just not as efficiently as soap and water which interacts with both heads and tails. What this means is that in order to be effective, the concentration of alcohol in the gel must be very high. Sanitisers on general sale are typically 60 – 80% alcohol, while those used in healthcare settings may be as high as 95%. This is not very good for the skin; frequent use of alcohol-based hand sanitisers will quickly dry out the skin of your hands, causing cracking and soreness. In addition, frequent use of alcohol-based hand sanitisers in hospitals has been linked to antibiotic resistance in faecal bacteria such as E. coli.
What about alcohol-free hand sanitisers? They are also less efficient than soap and water. They rely on antiseptic agents; two of the most common are benzalkonium chloride and triclosan. Benzalkonium chloride is widely used as a disinfectant in hospitals, but its use has been linked to the development of antibiotic resistance in MRSA. Triclosan breaks down into various compounds that accumulate in the environment and cause significant problems. Alcohol-free hand gels also have a shorter shelf-life and are more easily contaminated, so it’s important to keep an eye on the use-by date. Anyone who has been panic-buying alcohol-free sanitisers may well find that they end up having to throw them out if they can’t use them all by the use-by date.
So when are hand-gels useful? Basically for anyone who is in contact with people or animals, and for whom hand-washing is not always possible. This may include retail workers; veterinary workers; those in healthcare and those working with young children. Even in healthcare settings, though, staff are advised to wash their hands with soap and water whenever possible.
In conclusion, soap and water is more effective and better for your skin. It’s also better for your pocket – just compare the price of a bar of soap with that of a bottle of hand sanitiser.
There has been a lot of talk in the news in the last couple of days about how measures to deal with the spread of coronavirus COVID-19 are likely to move from the ‘containment’ phase into the ‘delay’ phase in the next few days. But what’s the difference?
Basically, the containment and delay phases do exactly what they sound like. Containment means that there are a small number of cases, and measures are taken to try and contain the virus and prevent it spreading. These include immediate testing of anyone at risk of being in contact with the virus; quarantine in isolation centres for those returning from high-risk areas; rigorous contact tracing for anyone who tests positive; and the closure and deep cleaning of any premises where there has been a confirmed case.
As the number of cases increases, the measures imposed during the containment phase may become unsustainable. As the virus is reported in more and more locations worldwide, it’s no longer possible to quarantine in government facilities everyone arriving in the country from places where there are confirmed cases. Quarantine is replaced with self-isolation, which of course relies on the compliance of those concerned. Contact tracing may also become impractical as the number of cases increase and there aren’t sufficient resources to trace and follow-up every single person that every person confirmed to have the virus has been in contact with.
With increasing spread of the virus, the closure and deep-cleaning of premises such as schools and healthcare facilities becomes not only impractical, but pointless, because it is likely that when such premises reopen, there will be more confirmed cases. Note that I am talking here about short term closures of a few days while premises are deep-cleaned, not the longer-term closure of places like schools to prevent pupil to pupil spread. More on that later.
Once it is apparent that containment has failed and the virus continues to spread, we enter the delay phase. Now, the aim is to slow the spread of the virus as much as possible. Measures during the delay phase include self-isolation for those who have the virus. Steps may also be taken to prevent or minimise situations where large numbers of people are in close proximity to one another. These may include the closure of schools and colleges; closure of entertainment venues such as cinemas; and the cancellation of large events such as sporting fixtures.
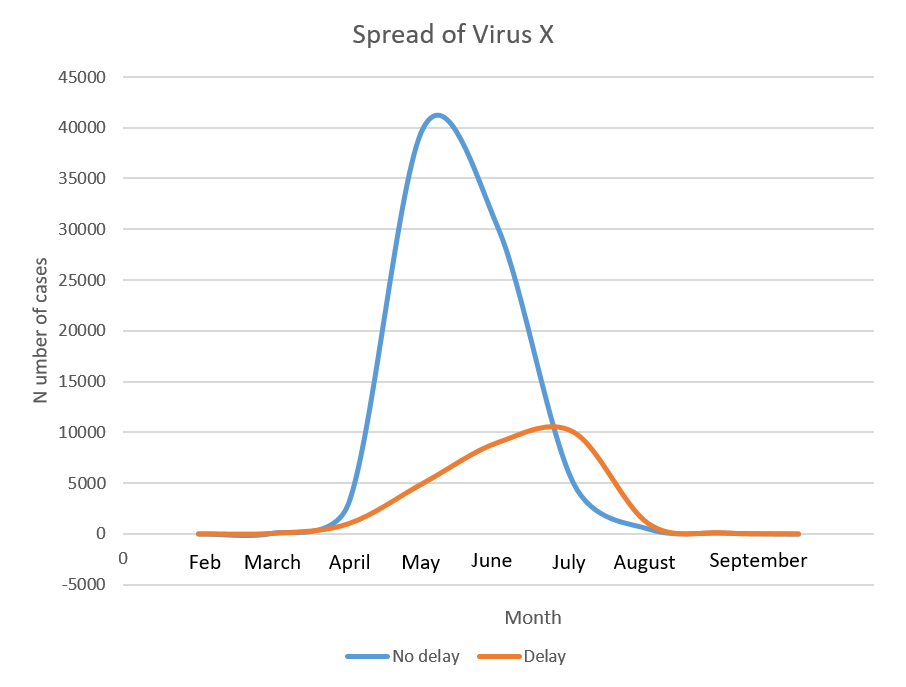
Measures taken during the delay phase will not stop the spread of the virus. So what’s the point? There are three main benefits. To illustrate these, the graph below shows the hypothetical spread of an imaginary virus I am calling X, which is spreading at a similar rate to that seen with COVID-19. The graph shows the number of cases by month, with and without delay measures.
The first benefit of delay measures is that the rate at which the number of cases increases is slower than it would be without. This means that the strain on the NHS would be far less than if there was a very rapid increase. It would also mean that the number of cases at any one time would be lower – again, reducing the strain on the NHS.
A second benefit is that cases would peak later in the year. The weather would (hopefully) be getting warmer, and there would be fewer other pathogens circulating, such as colds and flu. As I discussed in my earlier post, people fighting or recovering from other infections would be more susceptible to complications if they then caught COVID-19.
Thirdly, researchers and health professionals believe, based on the behaviour of other, similar coronaviruses, that COVID-19 will be less able to survive in warmer weather. This means that the time during which the virus can survive outside a host will be much reduced, making it harder for it to spread and potentially reducing the overall number of cases. I stress that at the moment, this last point is hypothetical, but it is a reasonable speculation based on evidence garnered from years of study of similar viruses.
Following my recent ‘Pathogens which really scare me’, I’ve been asked by quite a few people about two that did not make the list. One is Ebola, and I’ll talk about that in a later post. The other, yes you guessed it, Coronavirus COVID-19.
Microscopic view of Coronavirus, a pathogen that attacks the respiratory tract.
Don’t misunderstand me, I am absolutely NOT saying we shouldn’t be concerned. The emergence of any new pathogen, for which there is no vaccine or herd immunity, has to be of concern to anyone who calls themselves a scientist. And in my case, I also need to be concerned because I am asthmatic, and any respiratory infection puts me at risk of serious illness. But there is a difference between sensible concern and the hysteria which certain elements of the media are trying to promote.
As of 28th February 2020, there are around 84,000 confirmed cases and 2,860 confirmed deaths worldwide from COVID-19. That’s a death rate of 3.4% according to the WHO. But in actual fact, the death rate may well be a lot lower; there’s a high probability that many people have had COVID-19 and experienced such mild symptoms that they do not need to seek medical attention and are never tested. All the evidence indicates that for healthy people with no underlying risk factors, COVID-19 would cause a mild illness from which they would make a full recovery.
What about those in high risk groups then? As I said earlier, I am asthmatic so potentially at risk from serious complications if I get COVID-19. So, why am I not worried? Basically because there are plenty of simple, sensible precautions I can take which will minimise my risk. If you are an asthmatic reading this, and are concerned about COVID-19, you couldn’t do better than to read the excellent advice given by Asthma UK at https://www.asthma.org.uk/about/media/news/Coronavirus/.
COVID-19 is a virus, which means that it cannot reproduce outside a host organism, and the virus particles do not survive long outside a host. This means that basic hygiene measures can do a lot to halt the spread of COVID-19. Grandma was right when she said that ‘coughs and sneezes spread diseases’, and took you to task for not washing your hands. Covering your mouth when coughing, sneezing into a hanky (or the crook of your elbow if caught out without one) and washing your hands before meals and after going to the loo will do more to protect you than a mask. As a bonus, it will also significantly reduce your risk of other nasties such as colds, flu and Norovirus, any of which would massively increase your risk of serious complications if you caught COVID-19 while suffering/ recovering from them.
Another thing which helps protect me is that I’ve had my annual flu vaccine. What’s that got to do with it? Well, if you’ve had flu you will know how run-down it leaves you. During that recovery period, your immune system may be suppressed, leaving you at more risk of complications if you did get COVID-19. Last year I was unlucky enough to catch a strain of flu that the vaccine didn’t protect against. I was acutely ill with viral pneumonia for two weeks and it took a good couple of months for me to recover fully, during time which I would have been extremely vulnerable to complications if I had caught COVID-19. So does that mean the vaccine is useless? Absolutely not. last year I was unlucky, I just happened to be exposed to a strain of flu that the vaccine didn’t protect against. Getting my annual vaccine doesn’t entirely eliminate the risk of my getting flu, but it reduces it significantly.
Finally, I do everything I can to keep my asthma under control. Taking my preventer inhaler when I am well is a nuisance, but I do it. I monitor my symptoms and peak flow. I do my best to avoid triggers where I can, and if I get a cold or other respiratory infection, I double up on my preventer inhaler. I have a plan in place in case symptoms worsen.
Unfortunately, the media hysteria that I mentioned earlier may end up hindering people from taking basic precautions. A friend of mine posted on social media that it’s taken her several hours today to find a shop that had not sold out of hand gel. Ironically, the reason she was looking for hand gel was nothing to do with COVID-19. It was because she was getting ready to go to a ferret show, where using hand gel is an essential precaution against the spread of canine distemper – a pathogen that really does scare me (see my earlier post). A shortage of things like hand gel because people are stockpiling them may well increase the spread of colds, flu and Norovirus, any of which would make you more vulnerable to serious complications if you did get COVID-19.
My advice? Don’t ignore COVID-19, but don’t be misled by media panic. Take sensible precautions, as advised by the NHS at https://www.nhs.uk/conditions/coronavirus-covid-19/. If you have a health condition that makes you particularly vulnerable, like asthma, the best thing you can do is ensure that you take all medication as prescribed, and contact your GP or other health practitioner if your symptoms get worse. Just the same as you would if you got flu, or a common cold.
The saddest aspect of life right now is that science gathers knowledge faster than society gathers wisdom – Isaac Asimov
In February 2020, when I originally wrote this post, I stated that:
“there’s a bit of a health panic going on (understatement!). Masks are selling out, and I’ve just seen a post on social media from someone who had to visit five different stores in order to find hand-gel. But how scared should we really be of coronavirus COVID-19? As far as I’m concerned, there are plenty of candidates more deserving of our fear and respect. Here, in no particular order, are nine of the worst.”
It’s now nearly 2 years since I originally wrote this blog post, and a year since I last revisited it. a lot has happened in that time. When I initially wrote this post, COVID didn’t come close to making the list, because at the time, we still thought that quarantine and contact tracing would contain it. The SARS outbreak of 2002, and the 2009 H1N1 swine flu pandemic had lulled us into a false sense of security. Now it’s February 2022 and there are encouraging signs that we are finally coming out of the pandemic. I’ll post on that later. Meanwhile, in no particular order, here are my scariest pathogens.
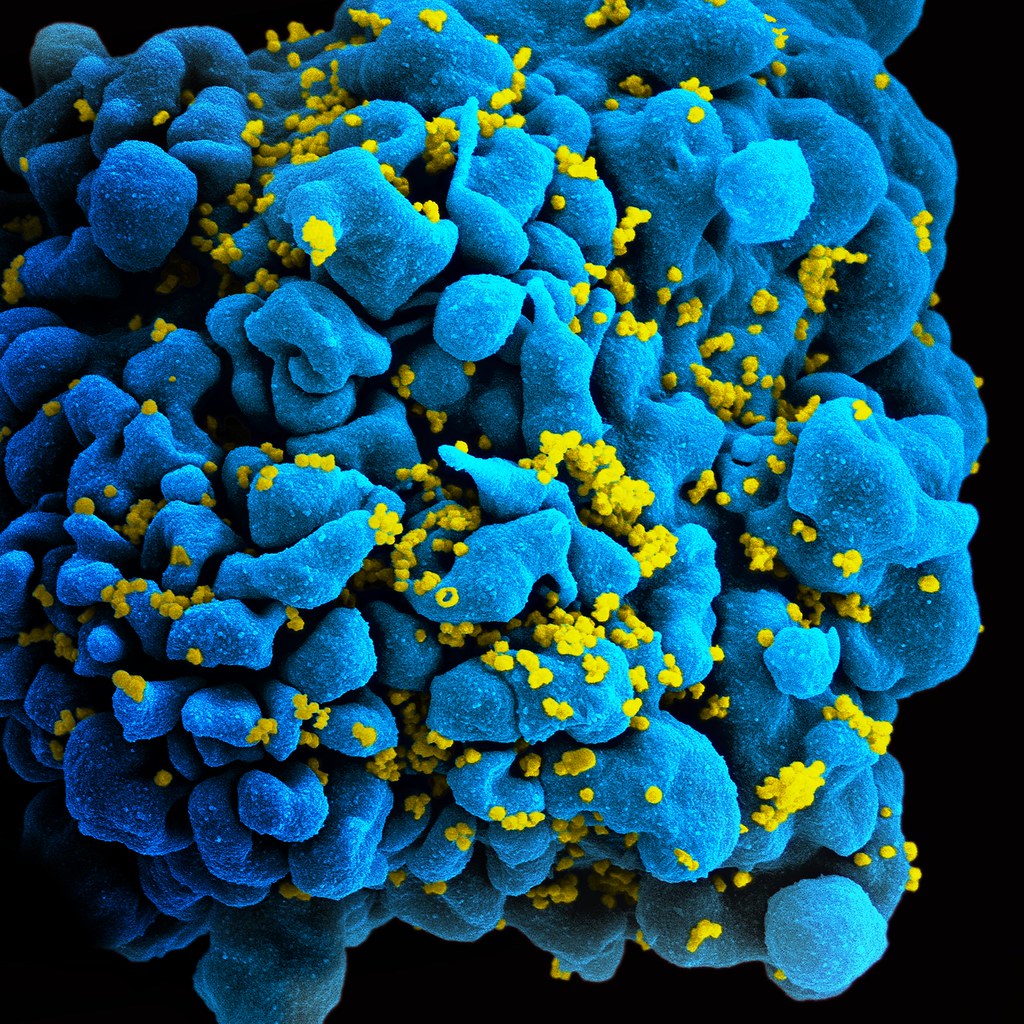
Helper T-cell infected with HIV
HIV
The human immunodeficiency virus (HIV) attacks the very cells that are meant to defend the body against it. It attacks cells which have the CD4 protein on their surface; these include helper T-cells which play a vital role in the immune system. Over time, the number of circulating helper T-cells decreases; when it drops below a certain level, the immune system effectively fails to function and the patient develops Acquired Immune Deficiency System (AIDS). AIDS has a high mortality rate since patients are unable to fight off serious infections.
But HIV has been conquered, right? Better awareness of the risks of unprotected sex; availability of condoms; provision of clean needles for IV drug users; all of these have helped to slow the spread of the infection. Effective anti-retroviral drugs (ARVs) mean that the disease can now be regarded as chronic; it rarely, if ever, progresses to AIDS.
Well, all of the above apply in developed, Western countries. In the developing world it’s a different story. Condoms are not always widely available, and in certain cultures or religions, their use is forbidden. ARVs are also not necessarily available. In some countries there is denial that HIV is what causes AIDS, meaning that governments refuse to provide access to treatment – this was the case for many years in South Africa.
But in the West we are OK, right? Wrong. HIV is a retrovirus, which means it writes its own DNA into that of infected cells. This means that it can never actually be eliminated from the body, and those infected must take ARVs throughout their lifetime. HIV also mutates rapidly, meaning that it develops resistance; new ARVs must be constantly developed to keep ahead of it. The fact that HIV continues to spread rapidly and go untreated helps it to keep mutating. How long can the drug developers keep ahead of it?
Malaria
Climate change means that currently malaria-free countries may develop conditions that allow the mosquito to breed
Malaria is caused by a plasmodium, a single-celled parasite spread through mosquito bites. According to the World Health Organisation (WHO), in 2018 there were approximately 228 million cases of malaria, with around 405,000 deaths. Malaria has a significant economic impact on countries where it is prevalent due to the cost of healthcare, loss of working days due to illness, and loss of worker productivity due to long-term effects.
The comparatively low death rate is due to the availability of effective anti-malarial drugs. However, malaria is becoming increasingly resistant to anti-malarial drugs, particularly in south-east Asia (Laos, Cambodia and Vietnam) where strains are emerging that are resistant to all currently available treatments. The development of resistant strains is partly due to the fact that organised criminal gangs in some countries are selling sub-standard or counterfeit drugs; these can only be detected using complex laboratory analysis.
A big problem with malaria is that there is no profit to be made from it. Developing new drugs is expensive, and the countries where malaria is prevalent cannot afford to pay the kind of prices big pharmaceutical companies want to charge in order to make a profit. Big pharma are not going to spend millions on developing a new anti-malarial just to make a loss on it, especially if the development of resistance means that after a few years, the drug will be ineffective. So, most of the research into new malaria treatments relies on subsidies from governments, NGOs and charitable donations. For example, one of the newest and most effective anti-malarials made it into clinical use because a partnership with the WHO meant that the manufacturing company could sell it at an affordable price and still make a profit. Fair play to the company concerned though, they did front up a significant amount of money in developing the drug. For the most part though, big pharma are putting their money into those diseases where there is most money to be made, such as cancer, diabetes and cardiovascular disease.
Lack of investment has also impeded development of an effective vaccine against malaria. A vaccine is currently undergoing pilot trials, but as yet there is no data as to how effective it is. Another problem with malaria is that unlike viral or bacterial infections, a patient who has had the disease and recovered does not develop immunity straight away. In fact, it takes multiple attacks of the disease for immunity to build up.
So, why does malaria worry me? Two words: climate change. The reason we don’t have malaria in the UK is that the conditions here are not suitable for the mosquitos which carry the parasite. Historically, malaria was actually very common in Europe and North America. In ancient Roman times, it was so prevalent in the city of Rome that it was known as ‘Roman Fever’. Climate change means that climates are warming up. Increasing incidents of flooding leave behind pools of standing water which may take a long time to drain away, providing a potential breeding ground for the malaria mosquito. As westerners, our neglect of malaria in favour of diseases which are more profitable or more likely to affect us may be about to turn around and bite us (pun intended).
Plague
Weaponisation is always a good indicator that a pathogen is scary. Plague is a highly infectious disease caused by the bacterium Yersinia pestis. Without treatment it has a high fatality rate. What makes plague particularly scary is the wide range of transmission routes. It is transmitted through airborne droplets; direct contact; indirect contact (e.g. with a contaminated surface); droplets from coughs or sneezes; contaminated food or water; faeces; and it is also transmitted by infected animals such as rats or fleas. Just about the only one missing from the list is sex, but I think that is because we can safely assume that if you get close enough to someone with plague to have sex with them, you are going to catch it.
Plague has a long history as a biological weapon. In ancient China, there are accounts of infected horse and cow carcasses being used to contaminate enemy water supplies. In medieval siege warfare, infected animal carcasses and even human corpses would be catapulted into enemy cities to infect the inhabitants. Some researchers speculate that this is how the Black Death first began to spread through Europe.
More recently, the Japanese used plague as a bioweapon in World War 2. The notorious Unit 731 developed bombs containing infected mice and fleas and used them against the Chinese in the city of Changde, contaminating the city and a wide area around it. They also carried out hideous experiments on prisoners to test the effectiveness of these weapons.
After WW2, both the US and USSR developed biological weapons based on plague, including strains which had been genetically engineered to create antibiotic resistance, and strains which had been combined with other bacteria such as diphtheria. Following the break-up of the USSR, it is possible that there are stocks of bio-weapons that are unaccounted for, and that could potentially fall into the wrong hands.
Still, shouldn’t be a problem because there’s a vaccine, and plague can be treated with antibiotics, right? Wrong. People are not routinely immunised against plague, and if it were used in, for example, bio-terrorism or a biological warfare attack on a civilian population, it would be too late for vaccination. Antibiotics may prove useless against genetically engineered strains. And, resistant strains have occurred naturally; for example, there have been outbreaks of a resistant strain in Madagascar as recently as 2017.
Anthrax
Anthrax spores can survive for decades in contaminated soil
Anthrax is another bacterial infection, caused by Bacillus anthracis. It can affect the skin, respiratory system or gastro-intestinal (GI) tract. Cutaneous (skin) anthrax is rarely fatal if treated, but is unpleasant and debilitating. Untreated, it causes death from septicaemia in about 20% of cases. Respiratory anthrax has a mortality rate of about 45% with treatment; untreated it is almost invariably fatal. GI anthrax is rare but has a mortality rate of 20-65%, depending on how quickly it is diagnosed and treated.
Anthrax can also affect cattle and sheep and is generally fatal because once symptoms appear, death is very quick, typically 2-3 hours. This means that both treatment and quarantine may be difficult. Infection can spread to other animals and humans through contact with infected animals or their remains.
The really scary thing about anthrax is that the bacteria can form spores, going into a sort of dormant state. These spores can survive for very long periods outside a host, for example in soil. In 1942, Gruinard Island off the coast of Scotland was used in a biological warfare trial involving anthrax bombs. Access to the island was forbidden until 1990, when it was re-opened to the public after a decontamination operation that had taken 4 years.
Anthrax was used as a biological weapon by Germany in WW1 and Japan in WW2 (Unit 731 again). In 1944 the British manufactured about five million animal feed pellets contaminated with anthrax; the plan was to drop them over Germany, infecting millions of cattle which would then infect humans. During the Cold War, the US and USSR continued to develop anthrax weapons.
The other really scary thing about anthrax is that the spores are relatively easy to cultivate; in theory, anyone with a moderate amount of microbiology and some fairly basic equipment can do it. This makes it attractive to bioterrorists as well as the military.
Smallpox
Smallpox causes pustules which leave patients disfigured for life
Smallpox is a highly infectious disease that is spread through airborne droplets, direct contact with an infected person or contact with a contaminated object. Before Edward Jenner’s discovery of vaccination, it was one of the leading killers in Europe. Those who survive smallpox are often left disfigured by scars or in some cases are blinded. It’s been used as a biological weapon since the 18th century; most recently, the USSR stockpiled tonnes of weaponised smallpox during the Cold War. And, of course, during WW2, our Japanese friends Unit 731 experimented with it extensively.
In 1980, the World Health Assembly officially declared that smallpox had been globally eradicated, thanks to a comprehensive world-wide vaccination program. Only two known samples remain, stored under the strictest security at the CDC in America and a high security bio-research facility in Russia. So, what’s the problem?
The problem is that word ‘known’. Actually, since 1980, other samples have turned up. For example, in 2014, six vials of smallpox dated 1954 were found in a cold storage facility in a Federal Drug Administration laboratory in the USA. They were transferred to the CDC and destroyed, but not before tests showed that the virus was still viable. Other samples may be hidden away in countries that would be less scrupulous. For example, can we really be certain that all virus stocks held in the former USSR have been accounted for?
Another problem is that even if all remaining samples are eradicated, smallpox could still be recreated. This was demonstrated in 2017 when Canadian researchers recreated the extinct horse pox virus, which is closely related to smallpox. Worryingly, they also demonstrated that this could be done by scientists without specialised knowledge, using basic lab equipment and at a relatively low cost; meaning that in theory at least, it could be done by bioterrorists or rogue nations.
Tuberculosis (TB) is an infectious disease caused by the bacterium Mycobacterium tuberculosis. It most commonly affects the lungs, attacking and destroying lung tissue. Scarring may occur where damaged lung tissue has healed. In some cases, other organs such as the brain or bones are affected.
It is thought that approximately 25% of the world’s population are infected with the TB bacterium. In 90% of cases, the infection is latent; the remaining 10% have active TB and are able to spread the infection through airborne droplets. Latent TB may become active due to immunosuppression, aging, malnutrition and certain diseases such as diabetes. At the present time, the biggest cause of latent TB becoming active is HIV.
M. tuberculosis is particularly dangerous because of its ability to evade the immune system. It is enclosed in a thick, waxy capsule which protects it from the chemicals that are used to destroy bacteria during phagocytosis. A M. tuberculosis bacterium that is engulfed by a macrophage will not be destroyed; in fact, it will reproduce inside the macrophage. This also prevents antigen presentation, so that the adaptive immune system is not activated.
The same waxy capsule makes M. tuberculosis very difficult to kill with antibiotics. Many antibiotics work by destroying bacterial cell walls; the waxy coating of M. tuberculosis is highly resistant to this. TB must be treated using specialised antibiotics; for example, ones which inhibit the synthesis of the waxy coating.
The rate at which M. tuberculosis develops antibiotic resistance is increasing, with a growing number of strains that are resistant to multiple drugs. Depending on the drugs used, treatment of TB with antibiotics takes 3-9 months, during which time the patient will usually be taking a combination of two or more antibiotics. Some patients stop taking medication before the infection has been eliminated, meaning that their treatable TB is at risk of becoming resistant. In poorer countries, the sale of sub-standard or counterfeit antibiotics also contributes to resistance.
Prior to 2005, all secondary school pupils in the UK were offered the BCG vaccine, which protects against TB. In 2005 this practice was discontinued due to the very low rates of TB in the UK. It was replaced with a targeted vaccination program in which the vaccine was offered only to those considered to be at risk of coming into contact with active TB. The effectiveness of the vaccine is variable. Studies have found that in the UK, the vaccine prevents TB infection in 60-80% of people. The duration of protection from the vaccine is also highly variable, meaning that some people who were vaccinated in childhood may no longer be protected. Outbreaks of TB in the UK are on the increase. This is due partly to immigration from countries where there are high rates of TB, and also due to the fact that more people with latent TB are developing active TB as a result of HIV.
So why does TB make the list? It’s difficult for the immune system to fight, and the vaccine may not offer effective protection. TB is developing antibiotic resistance at a worrying rate. There is a real risk that the rate of development of resistance will increase to a point where drug development cannot keep up, and strains emerge which are untreatable.
Influenza
While most people can fight off a bout of the flu, it should never be underestimated
They say familiarity breeds contempt, and nowhere is this truer than the humble flu virus. Typically, seasonal flu will cause an illness which, in healthy adults, is unpleasant but rarely fatal. However, even ‘normal’ seasonal flu can cause life-threatening complications in vulnerable people such as young children, the elderly, the immunosuppressed and those with pre-existing medical conditions.
Flu viruses mutate rapidly. However, simple mutation leads to relatively minor antigenic variation, so that individuals immune to the old strain may still have some immunity to the new one, which limits the spread of normal seasonal flu. A bigger problem is that influenza viruses can also undergo re-assortment; this occurs when different strains of the virus mix their genetic material and recombine it, resulting in a completely new virus. It happens when two different strains of virus infect the same host and leads to major genetic shifts and completely new antigens. When this happens, there is zero immunity in the population and available vaccines will not be effective; there is no herd immunity and this leads to a pandemic. Examples of this are the Spanish Flu pandemic of 1918-19 and the H1N1 Swine Flu pandemic in 2009.
The new viruses that result from re-assortment are not necessarily any more virulent than existing strains; the higher death rate from pandemic flu is because there is no vaccine or herd immunity, so vulnerable members of the population are unprotected. The Spanish Flu of 1918-19, which killed more people than WW1, was unusual because the mortality rate was highest among young, healthy adults. Recent research suggests that the virus triggered a cytokine storm. This is an abnormal immune response which caused activated immune cells to flood the lungs, leading to inflammation and build-up of fluid. Medical professionals at the time called this ‘dripping lung’. Patients either drowned in their own secretions or fell victim to secondary pneumonia. Ironically, the better your immune system, the more likely you were to suffer a cytokine storm, which is why the pandemic killed so many healthy adults.
More recent flu pandemics have not had the same mortality rate, partly because those viruses did not trigger a cytokine storm, and also because modern antibiotics were available to treat secondary bacterial infections. New anti-inflammatory drugs to treat cytokine storms are being researched; let’s hope they come into clinical use before a Spanish Flu type virus occurs.
Foot and mouth disease
The 2001 UK outbreak of FMD led to the culling of over 600 million sheep and cattle
You may be surprised to see that two of the pathogens that make this list are ones which do not even infect humans. Foot and mouth disease (FMD) is a highly infectious virus that affects cloven-hoofed animals such as cattle, sheep, pigs and goats. Although it is rarely fatal, it is extremely debilitating to infected animals and causes significant suffering. They suffer lameness due to blisters on the feet, and are unable to eat due to blisters in the mouth. This leads to severe weight loss, and animals take several months to recover. Milk production in females and fertility in males is also severely affected. Humans cannot catch FMD; when people claim to have had FMD, what they have actually had is hand, foot and mouth disease. This is a mild viral illness that typically lasts about a week.
FMD is highly infectious and can spread through direct contact between infected animals, or by indirect contact with contaminated items; for example, farm machinery or farmworkers’ boots and clothing. Meat products from infected animals can also carry the virus and it can even survive pasteurisation of milk. FMD has an incubation period of 1-12 days, during which the infected animal can pass the virus on to others. Because of the potential for rapid spread of infection, once it has been detected on a farm, all susceptible livestock must be culled and the carcasses burned or buried at an approved site.
FMD cannot infect humans, so why include it in my top ten? Quite simply because it has the potential to literally cripple a country, its infrastructure and its economy. The last major outbreak of FMD in the UK was in 2001 and lasted 9 months. Over 6 million cows and sheep were culled to try and halt the spread of the disease. Severe restrictions on the movement of animals meant that even farmers whose farms were not infected suffered significant financial losses. The tourism industry was also badly affected, with the number of overseas visitors to the UK dropping by 10%. All public rights of way were closed, and some major events were cancelled. It is estimated that the economic loss to agriculture was about £3.1 billion, with a loss of between £2.7 – 3.2 billion to other sectors of the economy such as tourism. The potential of FMD to damage economies and divert resources into combatting it could make it a potentially attractive agent for biological warfare or bioterrorism.
Canine distemper
Rhesus monkeys are the latest species, and the first primates, to become susceptible to CD
Canine distemper (CD) is an infectious disease that can infect a range of carnivores including canines (e.g. dogs, wolves, and foxes), mustelids (e.g. ferrets, mink and otters), big cats, seals, and skunks. Recently it has begun to cross into non-carnivores including Asian elephants, pandas and some species of primate. CD affects the respiratory and central nervous systems, and has a very high fatality rate. It is transmitted by droplets in the air or contaminated objects. The virus can survive for a fairly long time outside a host, for example on fur that has been shed by infected animals.
The CD vaccine is highly effective. CD does not affect humans, and does not have the potential to affect the economy the way FMD does. So why does CD scare me? Basically because of its remarkable ability to cross between different species. Within a relatively short time, CD has jumped from canines and mustelids into other carnivores, and then into non-carnivores. Most worrying of all is its recent jump into primates. Laboratory experiments have demonstrated that the strain which affects monkeys has the potential to interact with proteins on the cell membranes of human cells, meaning that in theory at least, CD could at some point cross into humans. The human population is mostly unprotected (immunity to measles does give some crossover protection against CD) and it would take time to develop an effective human vaccine. Most of the UK’s domestic dog population is vaccinated, but vaccination is not compulsory. Uptake of the vaccine among ferret owners is variable, and some vulnerable domestic pets such as skunks cannot currently be vaccinated. There is a huge reservoir of disease in the wild animal population, meaning that if the virus did become capable of infecting humans, the risk of a major outbreak would be significant, potentially resulting in a large number of deaths.
March 2021: Ironically, the COVID pandemic may actually result in a significant reduction in the risk of CD crossing into humans. In 2020, COVID-19 was discovered in mink on intensive fur farms in Scandinavia, resulting in a large-scale cull. The overcrowding in such farms provides ideal conditions for a pathogen to jump species: if COVID could jump from humans into mink, there’s a definite possibility of CD going the other way. If COVID means the end of intensive mink farming, then a significant risk will have been removed, as well as a major animal welfare issue.
COVID-19
Did not make the original list! I wrote the original in January 2020, when it still looked as though the virus might be containable. A year later, we were in lockdown #3, the UK death toll had passed 100,000, and new strains were emerging which became ever more infections. COVID-19 really is the gift that keeps on giving!
Now it’s February 2022 and the dominant strain is the omicron variant, which is highly infectious but causes only mild illness in the majority of people. This is likely to be due to the successful rollout of vaccines; but also that COVID-19 is following a well known evolutionary pattern by becoming more infectious but causing less severe disease. I will post more on this soon.
The COVID-19 virus
There is one good thing that has come out of the pandemic, and that is that immunology, and particularly vaccine science, has taken a huge leap forward. RNA vaccines have been in development for a number of years, but 12 months ago, not a single one had made it into clinical usage. Now, we have two RNA vaccines (Pfizer and Oxford/ AstraZeneca) being rolled out on a large scale, with others expected to gain regulatory approval in the next few weeks. It is my belief that the pandemic has advanced vaccine science in the same way that WW1 advanced radiography and blood transfusions; and WW2 advanced the use of antibiotics.
Ebola – the one that didn’t make it.
When I wrote the original blog post, a few people asked me why Ebola didn’t make the list of my top 10. It still doesn’t, and here’s why.
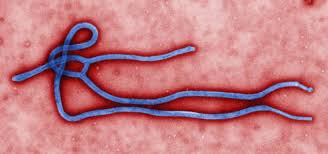
The distinctive ‘shepherd’s crook’ structure of the Ebola virus.
Ebola is one of a group of viruses called filoviruses. These have filament-like structures which coil to form a characteristic ‘shepherd’s crook’ shape. Like all viruses, Ebola invades cells and uses their organelles to reproduce. Ebola reproduces rapidly and efficiently. It triggers the release of chemicals that cause healthy cells to die; it also causes cell death by using up resources such as proteins at such a rapid rate that the cell is no longer able to maintain membranes and other structures.
Ebola causes damage and death to the endothelial cells that line blood vessels, leading to vascular instability – blood vessels literally disintegrate. At the same time it damages liver cells, impairing the clotting process. This results in massive and often fatal internal bleeding. It is able to evade the innate immune system by blocking the production of interferons. These are chemicals that are normally produced by cells which are infected with viruses; they signal natural killer cells (NKCs) to destroy the infected cell. Blocking the release of interferons allows Ebola to reproduce unchecked. The average death rate from Ebola is about 50%, but it can be as high as 90% depending on the strain. Death usually occurs as a result of hypovolemic shock – low blood pressure due to blood and fluid loss.
Remember when I said earlier that weaponisation is a good indication of how scary a pathogen is. Ebola is a devastating disease, highly infectious and with a high mortality rate. It’s a particularly gruesome pathogen as well – sufferers can literally bleed to death internally. This generates fear in the wider population; on the face of it, Ebola has all the makings of a weapon that would induce mass panic and terror as well as widespread death. But, Ebola has never been weaponised. And the reasons it has never been weaponised are the same as the reasons why it didn’t make my original ten.
Put simply, Ebola is too efficient for its own good. It reproduces so rapidly that it quickly destroys the cells it infects, killing its host in the process. The most deadly viruses are the ones that keep their hosts alive for long enough to infect as many others as possible. Even without intervention, Ebola outbreaks burn out relatively quickly.
Effective use of PPE and decontamination procedures mean that Ebola can be contained.
There are two other reasons Ebola still doesn’t make the top 10: transmission and survival outside a host. Ebola can only be transmitted through direct contact with the bodily fluids of an infected person: blood, saliva, vomit, semen etc. This means that use of PPE is highly effective in bringing an outbreak under control. In recent years, the importance of safe burial practices has also been recognised. This involves burying the dead as soon as possible; sealing the body inside leak-proof body bags; and ensuring that those handling the dead use PPE and hygiene measures effectively.
The other problem Ebola has is that it can only survive for very short periods outside a host, and is very easily destroyed by simple agents such as soap, bleach or detergent. The failure to weaponise Ebola (and trust me, several nations have tried!) is also down to its poor survival. You couldn’t put Ebola in a bomb, for example, because the detonation of the bomb would kill it off. A spray would also be of limited effectiveness, because the virus would only be viable for a very short period of time.